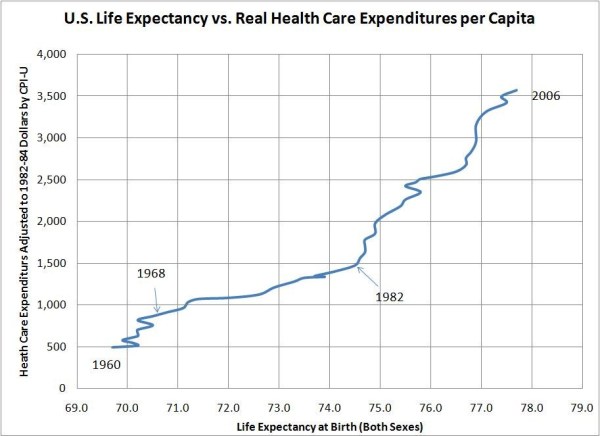
This question emerged unexpectedly from my post on US healthcare efficiency did not go off the rails until about 30 years ago. Lane Kenworthy posted the following graph to show that, when compared to all of 19 other wealthy OECD nations, US per-capita health care expenditures went through the roof while simultaneously delivering much smaller gains in life expectancy at birth.

My initial reaction was that something happened to accelerate the rate of spending increases in America. It did not occur to me that there had been a divergence in life expectancy improvement. However, taking the data apart revealed just the opposite: The rate of increase in real US per-capita health care expenditures has been steadily shrinking since at least 1960 but, starting in about 1983, America diverged downward from the peer nations in the rate of life expectancy improvements.
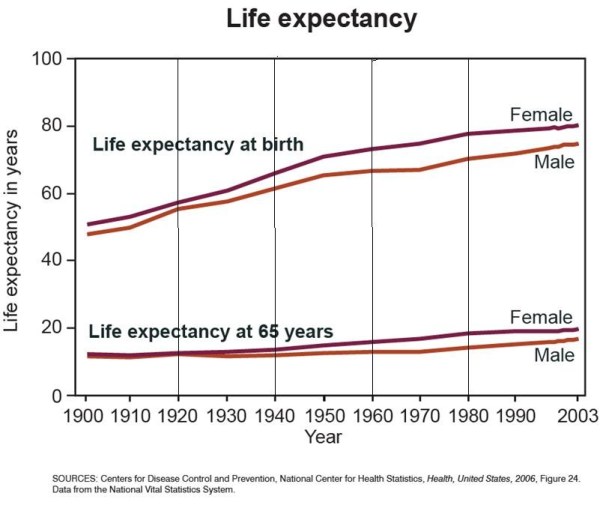
Digging a little deeper it appeared that most of the adverse divergence was attributable to females and that males continued to have life expectancy gains at about the same rate as in the recent past.
Why that happened was a complete mystery to me until the publication last month of U.S. Health in International Perspective: Shorter Lives, Poorer Health by the National Academy of Sciences. Hat tip Sabrina Tavernise at NYT. This is a monumental report of nearly 400 pages that is by no means focused on my question, "What's killing American females?" but there are clear partial explanations.
First, the study confirms that the US has been at or near the bottom in life expectancy and in the rate of increase in life expectancy and that the adverse divergence is almost entirely caused by US females.
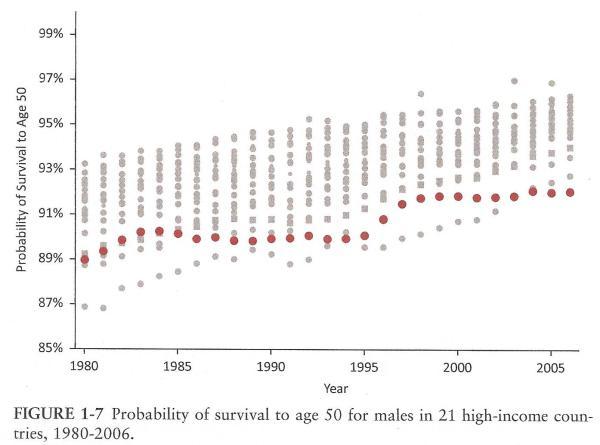
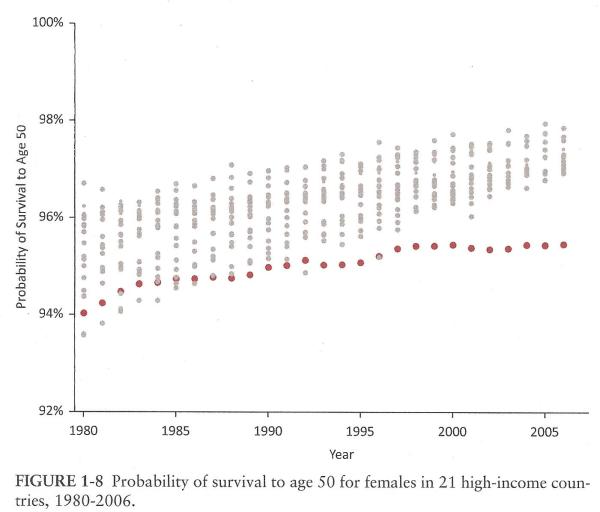
These charts show the probabilities of surviving to age 50, which the report tells us is the age range that primarily accounts for the US's life expectancy disadvantage. Indeed, after age 75, the life expectancy of Americans is higher than in peer nations. At 3.
One striking finding is that US death rates are higher than the mean of peer nations for almost all causes of death and is not near the best with respect to any cause of death. Table 1.2.
The report doesn't tell us what changed since 1983, but it does tell us which causes of death account for the poor showing of American females versus the mean of 16 peer nations in the 2006-08 time interval. Fully 37% of the excess deaths of American females occur from accidents and homicides, which are not normally thought of as "medical problems" that a better "health care system" might ameliorate.
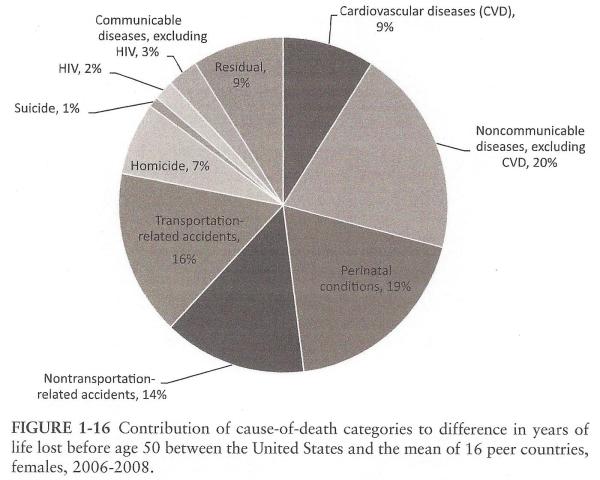
On the other hand, American females also lag their peers in deaths due to perinatal conditions, cardiovascular diseases, and other non-communicable diseases. Do American females have higher incidences of those maladies, or are they not getting as good treatment as in the peer nations? I don't think this report answers that.
Because the report provides only a snapshot from 2006-08, the report is unable to identify the causes of death most responsible for putting American females on their lower life expectancy trajectory in about 1983. Indeed, Recommendation 6 is to investigate how different policies may explain cross-national differences over time.
I'm sure this is not the most important health policy question of all time, but I found it intriguing and am glad to have partial answers. I'm even more pleased that the NAS and others are addressing in a thorough fashion what is making us sick and killing us and what policies have been found effective to improve our health.
None of this should distract us in any way from the disastrous growth since the early 1980s in per-capita health care spending that did not improve our lives. Well, I guess it improved the lives of health care vendors, but not my life. Or yours.
 Skeptic
Skeptic